Louisiana Snap Wage Verification Form
Louisiana Snap Wage Verification Form - The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the. Disposition mail the original to the employer *** or give to the. Snap applications can be submitted online and by mail or fax. Turn the form in to a local office; It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821;
Disposition mail the original to the employer *** or give to the. It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the. Snap applications can be submitted online and by mail or fax. Turn the form in to a local office;
Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; Disposition mail the original to the employer *** or give to the. Turn the form in to a local office; Snap applications can be submitted online and by mail or fax. It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the.

Printable Employment Verification Form Printable Word Searches
Snap applications can be submitted online and by mail or fax. Turn the form in to a local office; Disposition mail the original to the employer *** or give to the. Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; It is necessary to verify his/her current or anticipated income and health insurance coverage.

Louisiana Pathways Employee Verification Form 20202022 Fill and Sign
Disposition mail the original to the employer *** or give to the. Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; Snap applications can be submitted online and by mail or fax. The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the..
Snap Verification Documents Louisiana Complete with ease airSlate
It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the. Disposition mail the original to.
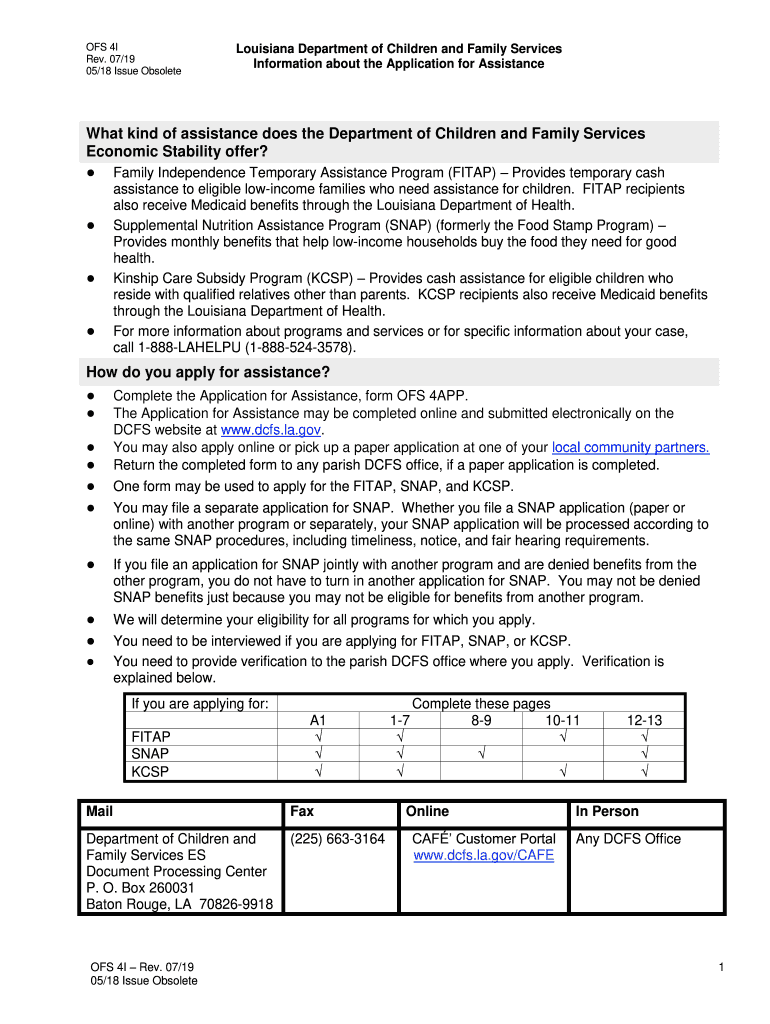
Supplemental Nutrition Assistance Program (SNAP) Louisiana Department
Disposition mail the original to the employer *** or give to the. Snap applications can be submitted online and by mail or fax. Turn the form in to a local office; Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; The bhsf employer form is used to request current, past, or anticipated wages and.
Printable Wage Verification Forms Printable Forms Free Online
The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the. It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Turn the form in to a local office; Snap applications can be submitted online and by mail or fax. Disposition.
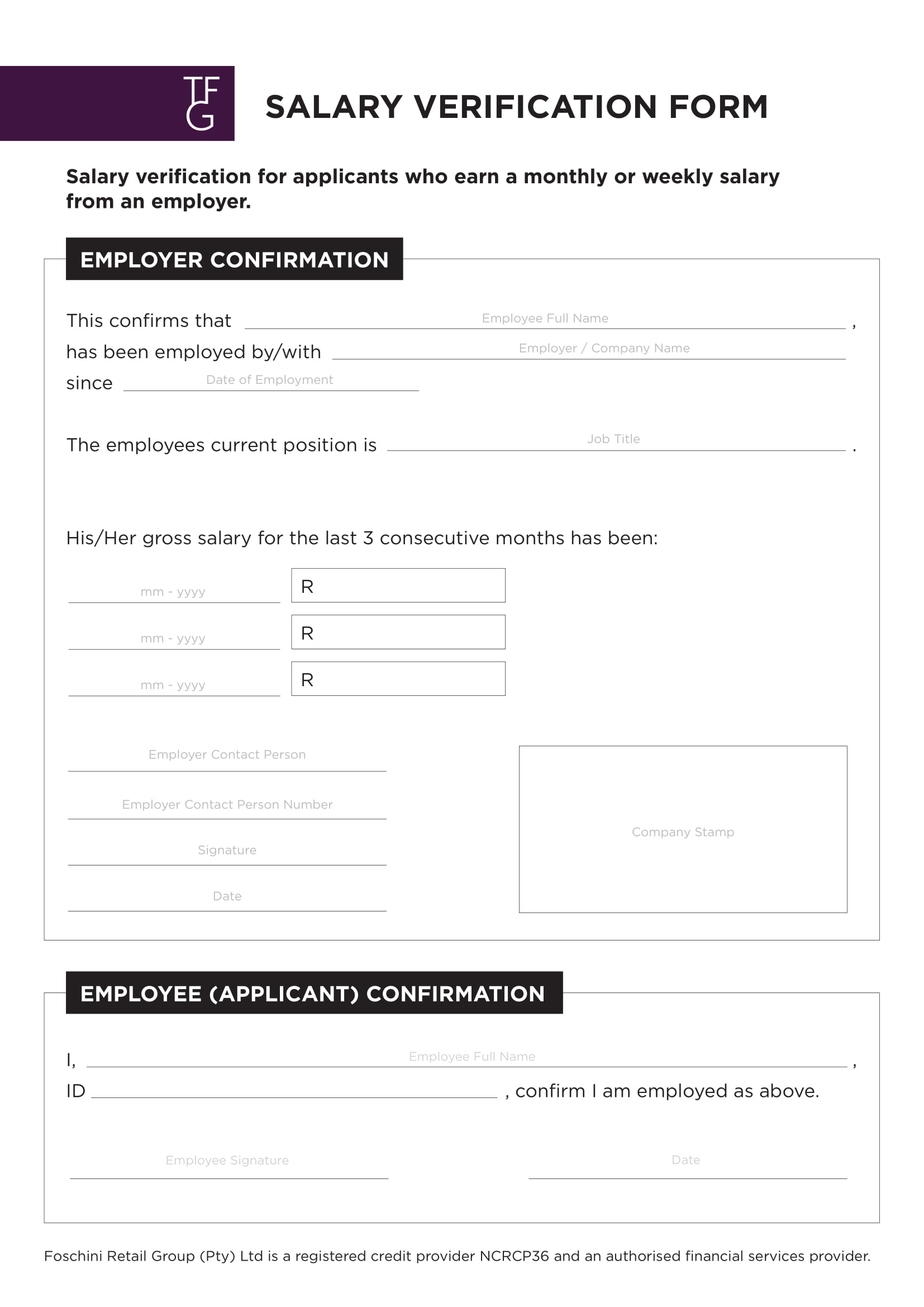
Snap Wage Verification Form Fill Out and Sign Printable PDF Template
It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Turn the form in to a local office; Snap applications can be submitted online and by mail or fax. The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the. Disposition.

Dss 8113 Fill out & sign online DocHub
Turn the form in to a local office; Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; The bhsf employer form is used to request current, past, or anticipated wages and health insurance coverage information for applicants whenever the. It is necessary to verify his/her current or anticipated income and health insurance coverage to.

Blank Snap Self Employment Verification Form PDF Economias
Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; Turn the form in to a local office; Snap applications can be submitted online and by mail or fax. Disposition mail the original to the employer *** or give to the. The bhsf employer form is used to request current, past, or anticipated wages and.
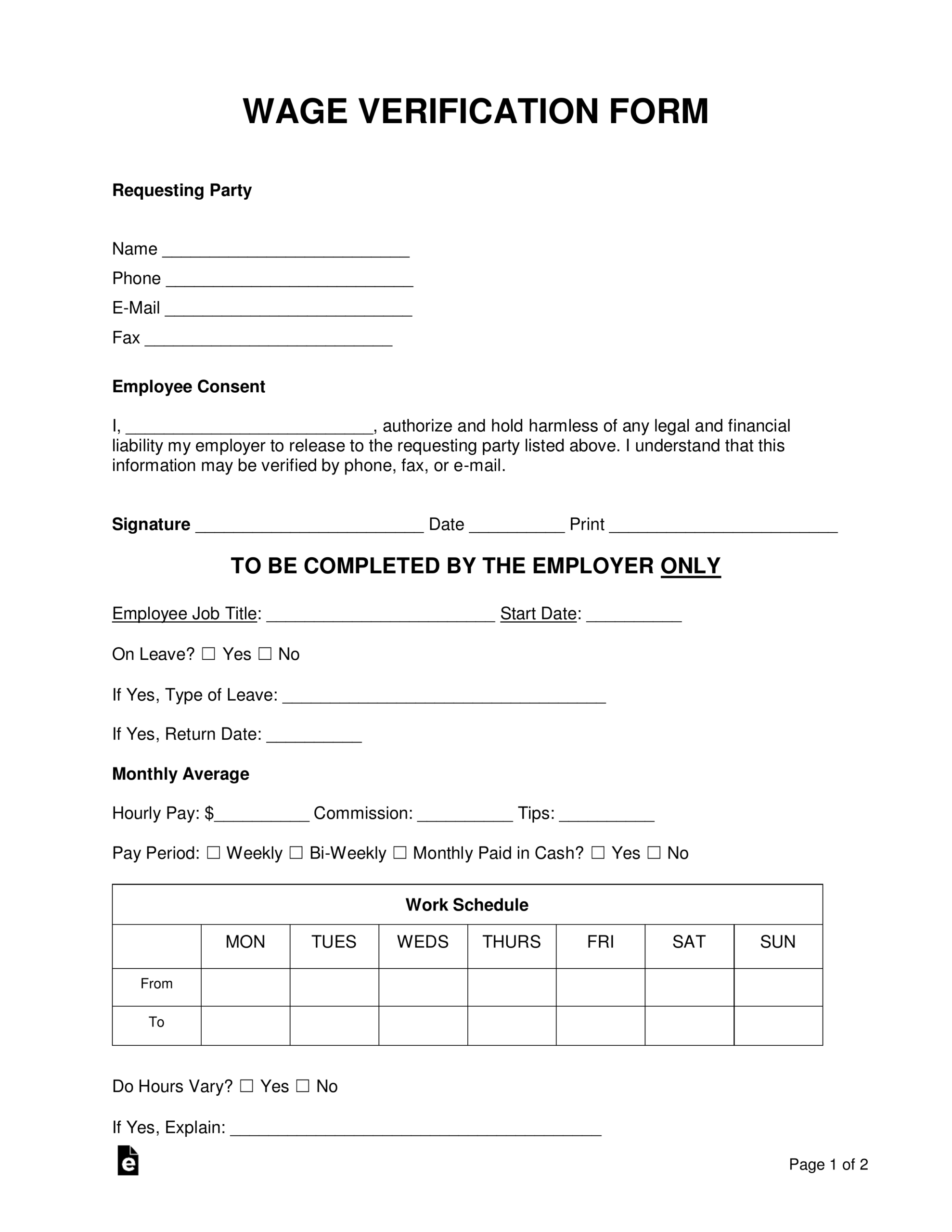
Wage Verification Form Template
It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Turn the form in to a local office; Disposition mail the original to the employer *** or give to the. Snap applications can be submitted online and by mail or fax. Mail it to dcfs civil rights section, p o box 1887,.

Wage for Food Stamps 20082024 Form Fill Out and Sign Printable PDF
Disposition mail the original to the employer *** or give to the. Snap applications can be submitted online and by mail or fax. It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility. Turn the form in to a local office; The bhsf employer form is used to request current, past, or.
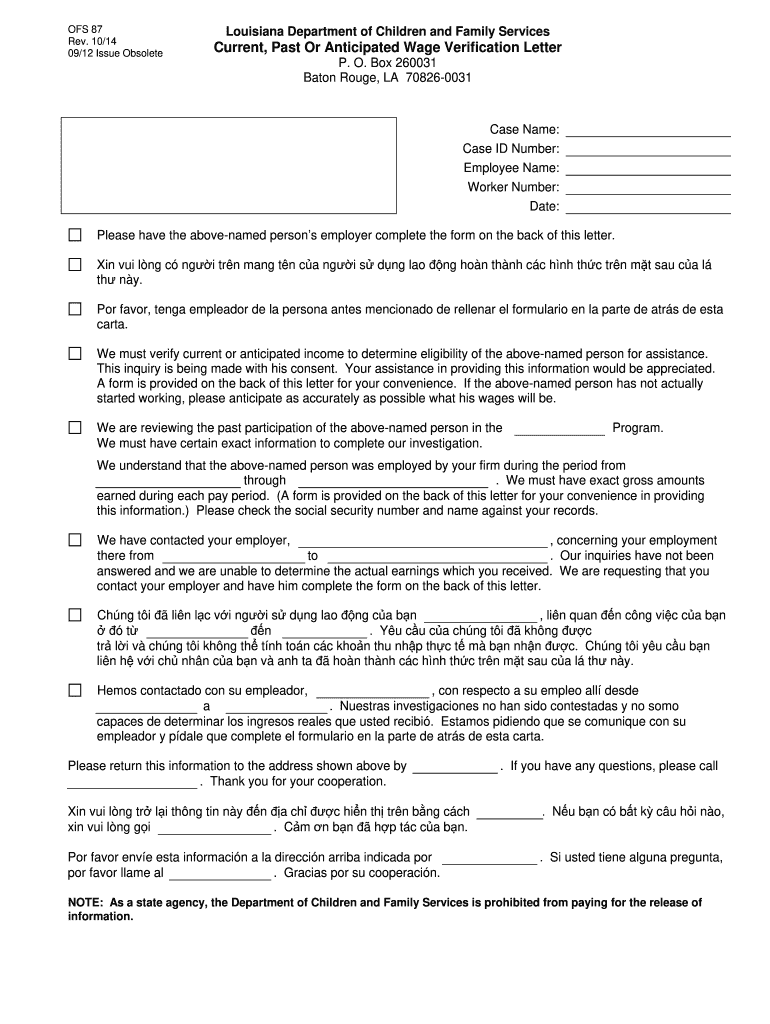
The Bhsf Employer Form Is Used To Request Current, Past, Or Anticipated Wages And Health Insurance Coverage Information For Applicants Whenever The.
Mail it to dcfs civil rights section, p o box 1887, baton rouge, la 70821; Disposition mail the original to the employer *** or give to the. Turn the form in to a local office; It is necessary to verify his/her current or anticipated income and health insurance coverage to determine medicaid eligibility.