Hill Rom Vest Order Form
Hill Rom Vest Order Form - The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. Prescription / order form phone 800.426.4224 fax to: It serves as a critical. (the prescriber must initial and date any revisions made after the prescriber has signed the order form). • sends completed form to hill. Fill out the form below and a member of the baxter respiratory health team will be in contact with you. Ordering the vest® system for home care use healthcare team responsibilities • completes the order form.
Ordering the vest® system for home care use healthcare team responsibilities • completes the order form. Prescription / order form phone 800.426.4224 fax to: (the prescriber must initial and date any revisions made after the prescriber has signed the order form). The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. Fill out the form below and a member of the baxter respiratory health team will be in contact with you. It serves as a critical. • sends completed form to hill.
It serves as a critical. Ordering the vest® system for home care use healthcare team responsibilities • completes the order form. • sends completed form to hill. The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. (the prescriber must initial and date any revisions made after the prescriber has signed the order form). Fill out the form below and a member of the baxter respiratory health team will be in contact with you. Prescription / order form phone 800.426.4224 fax to:
Hill Rom The Vest Airway Clearance System Model 205 277.5 Hrs Medsold
Prescription / order form phone 800.426.4224 fax to: • sends completed form to hill. Ordering the vest® system for home care use healthcare team responsibilities • completes the order form. Fill out the form below and a member of the baxter respiratory health team will be in contact with you. The purpose of this form is to facilitate the prescription.

HillRom 105 The Vest Airway Clearance System 10500 37.5 Hours
(the prescriber must initial and date any revisions made after the prescriber has signed the order form). It serves as a critical. The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. Prescription / order form phone 800.426.4224 fax to: • sends completed form to hill.

Hill Rom The Vest Airway Clearance System, For Clinical at Rs 550000
• sends completed form to hill. (the prescriber must initial and date any revisions made after the prescriber has signed the order form). Fill out the form below and a member of the baxter respiratory health team will be in contact with you. Prescription / order form phone 800.426.4224 fax to: Ordering the vest® system for home care use healthcare.

Hillrom Vest 105 Hillrom Airway Clearance Vest Medafore
• sends completed form to hill. Fill out the form below and a member of the baxter respiratory health team will be in contact with you. The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. Prescription / order form phone 800.426.4224 fax to: (the prescriber must initial and date any.

Used HILLROM The Vest Airway Clearance System Model 105 Airway
Prescription / order form phone 800.426.4224 fax to: (the prescriber must initial and date any revisions made after the prescriber has signed the order form). It serves as a critical. Ordering the vest® system for home care use healthcare team responsibilities • completes the order form. The purpose of this form is to facilitate the prescription and order process for.

Hillrom Vest 105 Hillrom Airway Clearance Vest Medafore
The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. Fill out the form below and a member of the baxter respiratory health team will be in contact with you. Ordering the vest® system for home care use healthcare team responsibilities • completes the order form. Prescription / order form phone.
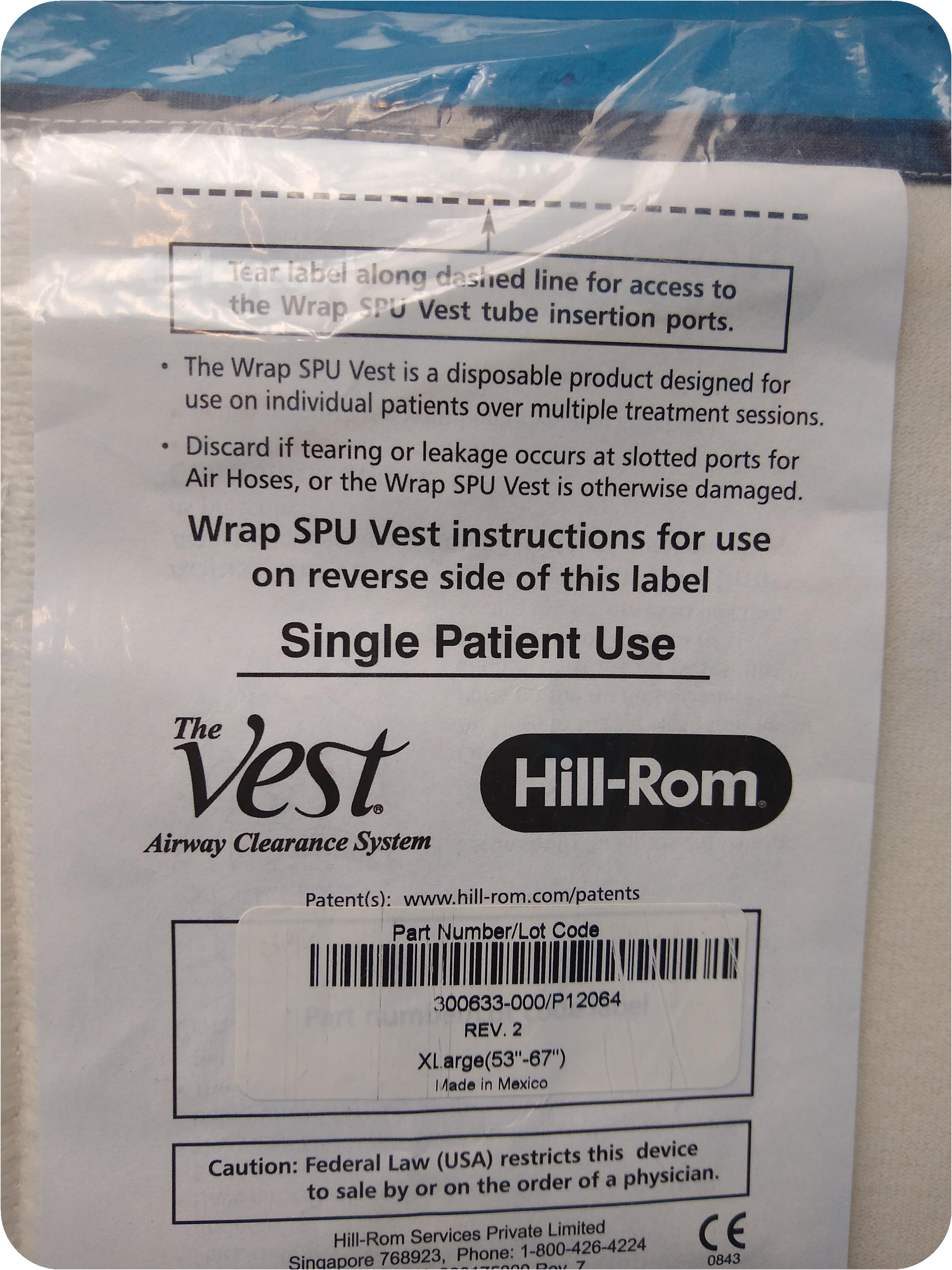
tekyard, LLC. 246960HillRom 300633000/P12064 SPU Vest Extra Large
(the prescriber must initial and date any revisions made after the prescriber has signed the order form). Fill out the form below and a member of the baxter respiratory health team will be in contact with you. It serves as a critical. • sends completed form to hill. The purpose of this form is to facilitate the prescription and order.

HillRom 105 The Vest Airway Clearance System 10500 37.5 Hours
(the prescriber must initial and date any revisions made after the prescriber has signed the order form). It serves as a critical. • sends completed form to hill. Fill out the form below and a member of the baxter respiratory health team will be in contact with you. Ordering the vest® system for home care use healthcare team responsibilities •.

The Vest Airway Clearance System Hillrom Vest 205
The purpose of this form is to facilitate the prescription and order process for the vest® airway clearance system. (the prescriber must initial and date any revisions made after the prescriber has signed the order form). • sends completed form to hill. It serves as a critical. Ordering the vest® system for home care use healthcare team responsibilities • completes.

Cystic Fibrosis Vest / The Vest System Model 105 Hillrom / Cystic
Fill out the form below and a member of the baxter respiratory health team will be in contact with you. It serves as a critical. Prescription / order form phone 800.426.4224 fax to: (the prescriber must initial and date any revisions made after the prescriber has signed the order form). Ordering the vest® system for home care use healthcare team.
Ordering The Vest® System For Home Care Use Healthcare Team Responsibilities • Completes The Order Form.
Prescription / order form phone 800.426.4224 fax to: • sends completed form to hill. It serves as a critical. Fill out the form below and a member of the baxter respiratory health team will be in contact with you.
The Purpose Of This Form Is To Facilitate The Prescription And Order Process For The Vest® Airway Clearance System.
(the prescriber must initial and date any revisions made after the prescriber has signed the order form).