Community Health Choice Prior Authorization Form
Community Health Choice Prior Authorization Form - All requests for prior authorization require submission of supporting clinical records. Prior authorization request form please complete this entire form and fax it to: Please check the formulary under the pharmacy. Providers must submit the prior authorization request form. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. The form must include the following information:
The form must include the following information: All requests for prior authorization require submission of supporting clinical records. Please check the formulary under the pharmacy. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. Prior authorization request form please complete this entire form and fax it to: Providers must submit the prior authorization request form.
The form must include the following information: All requests for prior authorization require submission of supporting clinical records. Prior authorization request form please complete this entire form and fax it to: Providers must submit the prior authorization request form. Please check the formulary under the pharmacy. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests.

Keystone First Community Health Choice Prior Authorization Form
Providers must submit the prior authorization request form. Please check the formulary under the pharmacy. The form must include the following information: All requests for prior authorization require submission of supporting clinical records. Prior authorization request form please complete this entire form and fax it to:

Sc Prior Authorization Fill Online, Printable, Fillable, Blank
Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. The form must include the following information: All requests for prior authorization require submission of supporting clinical records. Please check the formulary under the pharmacy. Prior authorization request form please complete this entire form and fax it to:
FREE 8+ Sample Prior Authorization Forms in PDF MS Word
Please check the formulary under the pharmacy. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. All requests for prior authorization require submission of supporting clinical records. Prior authorization request form please complete this entire form and fax it to: Providers must submit the prior authorization request form.

Fillable Online Prior Authorization Form Providers Prestige Health
Please check the formulary under the pharmacy. The form must include the following information: All requests for prior authorization require submission of supporting clinical records. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. Prior authorization request form please complete this entire form and fax it to:
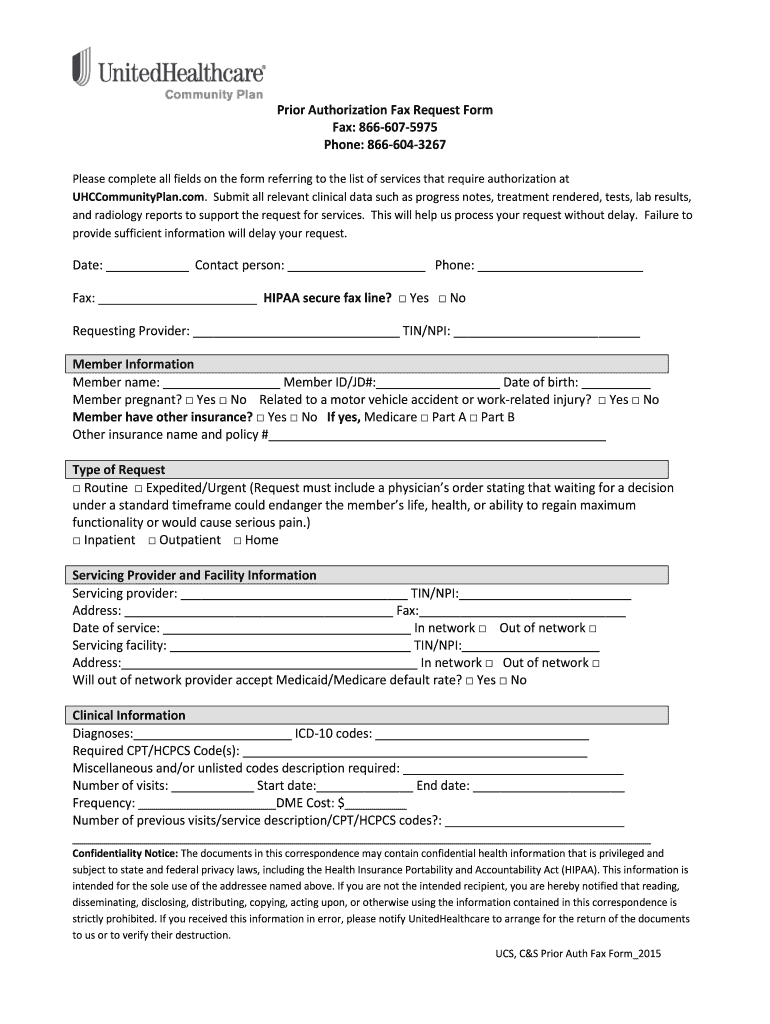
United Healthcare Community Plan Pre Authorization Form
All requests for prior authorization require submission of supporting clinical records. The form must include the following information: Please check the formulary under the pharmacy. Providers must submit the prior authorization request form. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests.
Free California Medicaid Prior Rx Authorization Form Pdf Eforms
Prior authorization request form please complete this entire form and fax it to: The form must include the following information: Please check the formulary under the pharmacy. Providers must submit the prior authorization request form. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests.
UHC prior authorization form Free Job Application Form
The form must include the following information: Please check the formulary under the pharmacy. Prior authorization request form please complete this entire form and fax it to: Providers must submit the prior authorization request form. All requests for prior authorization require submission of supporting clinical records.
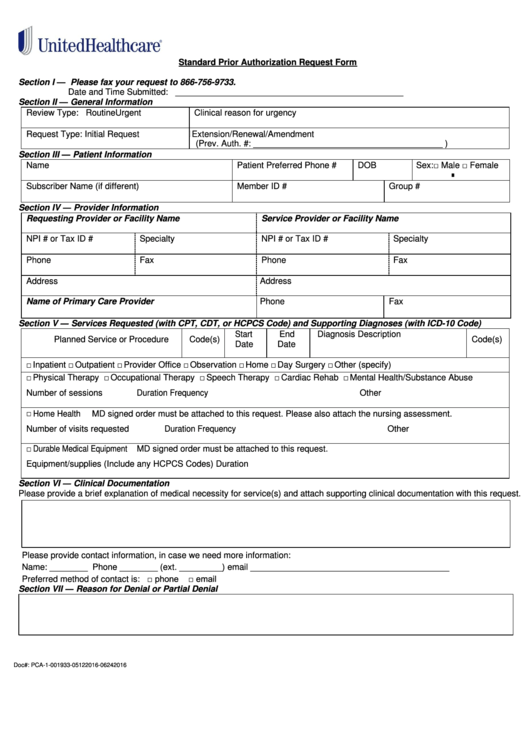
Fillable Standard Prior Authorization Request Form United Healthcare
All requests for prior authorization require submission of supporting clinical records. The form must include the following information: Providers must submit the prior authorization request form. Please check the formulary under the pharmacy. Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests.
Authorization Fax Request Form Fill Online, Printable, Fillable
Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. The form must include the following information: All requests for prior authorization require submission of supporting clinical records. Prior authorization request form please complete this entire form and fax it to: Please check the formulary under the pharmacy.
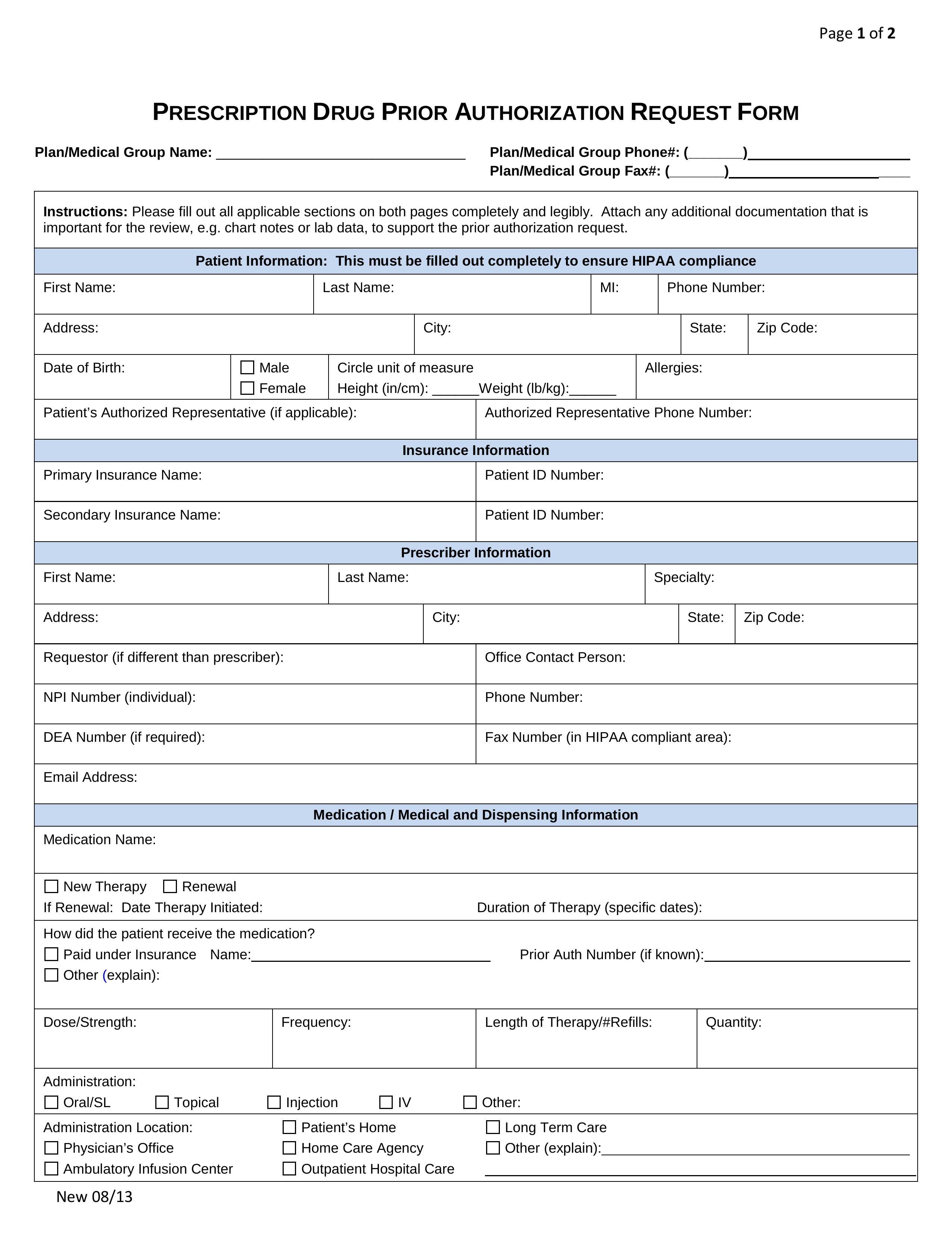
Free Prior (Rx) Authorization Forms PDF eForms
The form must include the following information: Please check the formulary under the pharmacy. Prior authorization request form please complete this entire form and fax it to: All requests for prior authorization require submission of supporting clinical records. Providers must submit the prior authorization request form.
All Requests For Prior Authorization Require Submission Of Supporting Clinical Records.
Please check the formulary under the pharmacy. Prior authorization request form please complete this entire form and fax it to: Dhs prescription form for motorized wheelchairs is necessary for all power wheelchair and scooter requests. Providers must submit the prior authorization request form.